Many of us have had friends or loved ones that have been diagnosed with some form of cancer and have received treatment such as chemotherapy. It is common for cancer patients that receive chemotherapy to become very ill from the medicine they are taking to treat their cancer. They may lose all of their hair, have trouble eating because of stomach problems, and are more likely to become very ill from an infectious disease. These negative side effects from chemotherapy treatment occur because they target fast-growing cells like cancer cells, but also kill fast-growing cells in the hair, the lining of the stomach, and white blood cells. Despite this, cell death is a normal process in our bodies.
Several billions of normal cells die and are replaced by new cells in the human body every day. This is part of our body’s homeostasis, which means the tendency for living systems to maintain stability. This turnover of old cells in favor of newer cells ensures that our body continues to function normally. Now, most of these daily demises go unnoticed by our immune system and are called tolerogenic cell death. This means that these cells die and are replaced without activating white blood cells or an inflammatory response. In contrast, when cells die due to an infection or disease, an immune response occurs so that pathogens can be eliminated from the body. The immune response is a process when our body tries to recognize and fight against a substance that appears foreign or harmful. This includes the generation of memory against the pathogen so that white blood cells (immune cells) can recognize these foreign invaders later. Cancer cells, however, are altered versions of our own cells so they are not considered foreign and therefore do not activate the immune system. So, it is typically easy for them to escape from the immune system and can divide and grow freely without consequence. Since our immune cells are so adept at recognizing foreign pathogens, it would be useful if they could recognize and respond to cancer cells as well. This could result in an earlier diagnosis of cancer and an improved treatment regimen with fewer negative side effects. So the million-dollar question is – how can we make our immune system recognize and respond against these cancer cells?
Until recently, cancer treatments were developed with the main goal of killing cancer cells. Chemotherapies have been very successful for many cancers in this regard and thus remain front-line therapies today. However, as mentioned previously, chemotherapies are indiscriminate when it comes to rapidly dividing cells leading to severe side effects such as weakened immune systems. Despite some therapies having greater or equal cancer-killing capabilities, they might not have better outcomes for the patient than less potent chemotherapies. For example, two chemotherapy drugs – oxaliplatin and cisplatin, which have similar chemical properties as well as similar killing efficacy, show different outcomes in cancer patients. In gastric cancer as well as colorectal cancer patients, oxaliplatin is shown to be superior as compared to cisplatin. What is the reason behind this discrepancy?
The answer can be explained by the phenomenon called “immunogenic cell death” (ICD).
Immunogenic cell death (ICD), simply put, means cell death that induces an immune response. As mentioned before, we have billions of cells dying daily without inducing any immune response, so how is this immunogenic cell death different? Unlike the daily turnover, upon some chemotherapy treatments, cells die while secreting “danger signals”. These danger signals help alert the immune system and direct immune cells towards them to destroy the perpetrator, for example, the cancer cell. Danger signals are released in space and time-dependent manner, that is, some are present on the surface of cells, some are secreted outside of the cell, and some are released within minutes to days. These are also called “damage-associated molecular patterns” (DAMPs). These DAMPs play a key role in alerting different parts of the immune system.
The reason some chemotherapies or cancer therapies are superior to others, in general, can be explained by whether or not these DAMPs are released. Cancer cell death from chemotherapy treatment can activate the immune system in the same way that cell death from infection does, by secreting danger signals. Different cancer therapies can generate a unique panel of danger signals. For example, chemotherapies, radiation therapy, and photodynamic therapies elicit unique DAMP signals which result in a variety of immune responses. These unique DAMPs or ICD signatures are also called ICD “hallmarks”.
The most common ICD hallmarks noted to date in multiple therapies are Calreticulin (CALR), ATP, and HMGB1 (Figure 1). CALR is generally present inside the cell. But upon ICD, CALR translocates to the outside of a dying cell and it functions as an “eat me” signal for immune cells called dendritic cells. Dendritic cells are like PacMan of the immune system, they swallow foreign substances that come in their way. When these dendritic cells see CALR on the surface of the cells, it’s their signal for danger, so they gobble up those cells. Similar to CALR, ATP is released outside the cell upon ICD and acts as a “find me” signal for the dendritic cells. It induces the attraction of these immune cells to the tumor site. HMGB1 is considered to be a late marker of ICD and its release from inside the nucleus, or the center of the cell where DNA is found, to the outside of the cell occurs upon ICD. Along with CALR and ATP, HMGB1 activates these dendritic cells, which eat the cancer cells and present small parts of these cancer cells (antigens) on their cell surface to other immune cells such as T cells. These small parts of cancer cells or antigens are like IDs that immune cells use to track them out. T cells are a type of white blood cell, which function as specifically trained detectives. These cells investigate the evidence provided by the dendritic cells and specifically target and kill the cancer cells. In this way, the danger signals from cells undergoing ICD can help activate the immune system.
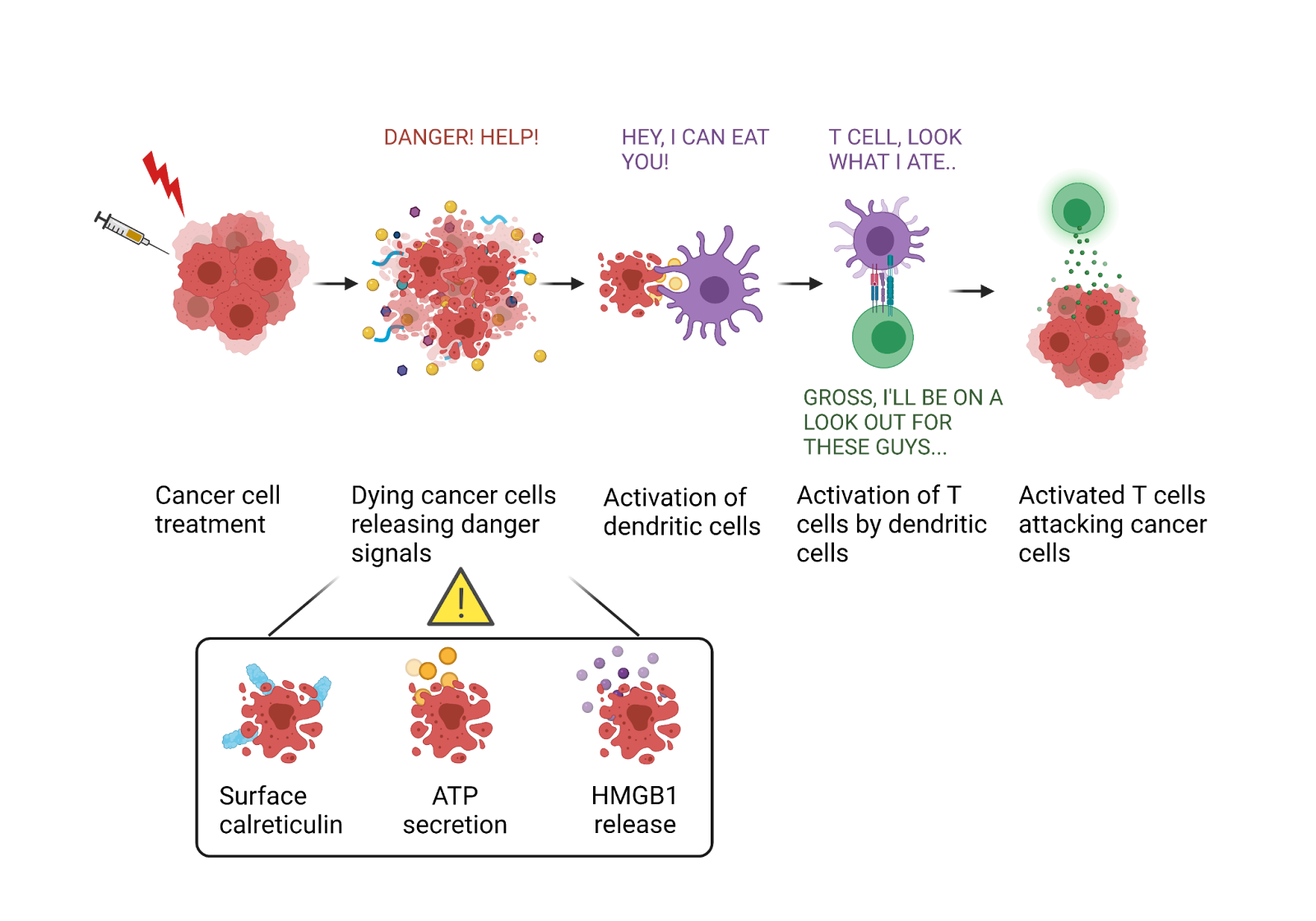
Figure 1. Immunogenic cell death of cancer cells. In response to ICD inducing cancer treatments, cancer cells die immunologically by releasing different danger signals such as surface calreticulin expression, ATP secretion, and HMGB1 release. These signals together can activate phagocytic immune cells such as dendritic cells. These cells further activate and alert other immune cells such as T cells. Together, ICD can induce an anti-tumor immune response which can attack and kill cancer cells.
The ‘gold standard’ experiment to confirm that specific chemotherapy will result in ICD involves injecting mice with chemotherapy-treated dying cancer cells. This is similar to a vaccine because it exposes immune cells to the weakened cancer cells so that the immune system will recognize them later, but they won’t be able to cause any damage in the meantime. Then the mice are challenged 1 week later with the same cancer cells, but this time they are alive and could cause damage. If these dying cancer cells are undergoing ICD, they will release different danger signals, activating the immune system against cancer. So, when we challenge mice with intact-live cancer cells, the immune system which has already been activated against this cancer, will immediately take charge and prevent the growth of cancer. On the other hand, if the dying cancer cells are not undergoing ICD, the immune system will not recognize the live cancer cells during the challenge and which will result in cancer growth. This also means that it was a bad vaccine. The success of ICD upon cancer therapy has been attributed to the activation of immune cells including T cells which constitute the main players of the anti-tumor immune response (Figure 1). These responses have also been shown to generate ‘immunological memory’ which can prevent the recurrence of certain cancers.
The discovery of ICD has revolutionized the field of cancer therapies by changing our understanding and evaluation of cancer therapies drastically. Today, it is not enough that cancer treatment kills the cells. It is more important whether or not it is activating the immune system against cancer. Currently, studies are underway to determine the potential to use these ICD-based cancer vaccines for the treatment of cancer.
Figure created with BioRender.com
Feature image from sciencephotolibrary.com
