Have you ever seen a movie or read a book that had a twist ending where the supposed “good guy” was the villain or an anti-hero? This plot can occur during the body’s immune response. Our immune systems are intended to defend us against pathogens, such as SARS-CoV-2, but sometimes it accidentally turns on our own body to cause harm. In the case of long COVID, researchers have recently seen evidence that this is the plotline unfolding with autoantibodies playing a starring role. Before we dive into this research, let’s walk through some background information on our main characters: long COVID and autoantibodies.
Long COVID results in symptoms that linger in individuals for weeks or months after suffering from SARS-CoV-2 infection. Some of these symptoms include loss of smell and taste, fatigue, shortness of breath, brain fog, and blood clots. Long COVID can ultimately result in damage to multiple organs including the brain, heart, lungs, kidneys, and vascular system. And this disease doesn’t occur only in hospitalized individuals – prolonged symptoms have been documented in those who had just mild cases of COVID-19.
New research suggests that during long COVID autoantibodies might be key drivers of pathology. To understand autoantibodies, we first have to talk about antibodies. Antibodies are proteins produced by the immune system that recognize foreign substances and pathogens like SARS-CoV-2. During infection, antibodies are key to fighting pathogens, they have various functions including neutralization of pathogens thus rendering them ineffective. Most of the time, antibodies only attack and neutralize foreign proteins. But in some cases, the immune system makes the mistake of recognizing proteins from our own bodies as a threat. When this happens, the immune system generates autoantibodies that target and attack proteins expressed by our own tissues. Thus, rather than being a hero, the immune system (specifically the autoantibody) becomes the villain.
ACE2: a gatekeeper of inflammation
Arthur, et al. set out to understand the role of autoantibodies against the host protein, ACE2, following SARS-CoV-2 infection and how these autoantibodies might contribute to long COVID. ACE2 was of particular interest to the researchers for multiple reasons. First, ACE2 is a host protein that SARS-CoV-2 recognizes and uses to enter our cells with its viral spike protein. Think of ACE2 as the lock on a door and the viral spike protein as the key that SARS-CoV-2 uses to unlock the door and access our cells. Once inside, SARS-CoV-2 hijacks our cell’s machinery to replicate itself and cause disease. In addition, ACE2 has a role outside of infection to decrease immune activity and prevent self-inflicted damage to cells. A loss of ACE2’s normal function can result in a heightened inflammatory state.
During SARS-CoV-2 infection, we generate antibodies against the viral spike protein to help neutralize and clear infection. However, it is possible for anti-idiotypic antibodies to also form. Anti-idiotypic antibodies are specific to and recognize a region of host antibodies, in this case the antibodies against the viral spike protein generated during acute infection. These anti-idiotypic antibodies are also capable of recognizing the viral protein’s original binding partner, ACE2. In other words, we can develop autoantibodies targeting ACE2.
Over the course of acute SARS-CoV-2 infection, ACE2 becomes bound by the virus, preventing it from carrying out its normal anti-inflammatory job. This in turn can result in immune system-mediated damage. Thus, COVID-19 pathology is often characterized by heightened levels of inflammation. A state of hyper inflammation is still observed during long COVID suggesting ACE2’s role is compromised. Armed with this information, Arthur, et al. hypothesized that in long COVID patients the immune system generates autoantibodies against ACE2 in the form of anti-idiotypic antibodies that target the anti-spike protein antibodies generated during acute infection.
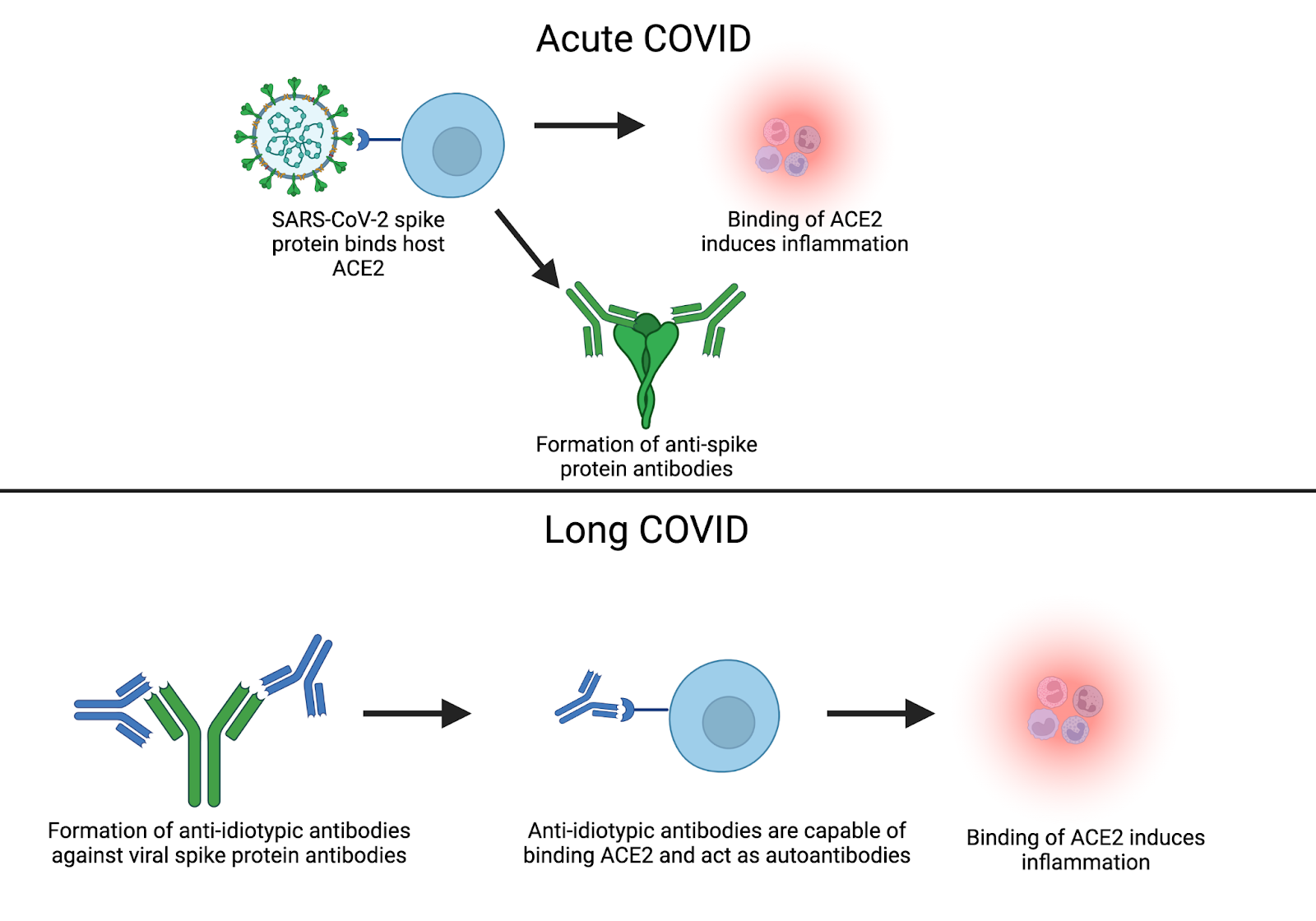
Figure 1: Arthur, et al working hypothesis. Binding of ACE2 by the SARS-CoV-2 spike protein leads to increased inflammation during acute infection. Antibodies against the SARS-CoV-2 spike protein are generated during acute infection. ACE2 autoantibodies are generated in the form of anti-idiotypic antibodies in response to spike protein antibodies. Binding of ACE2 by ACE2 autoantibodies leads to increased inflammation during long COVID. Created with BioRender.com
To explore this hypothesis, human serum and plasma samples were collected for analysis. The cohort was broken down into four groups: Inpatient with positive PCR test, Outpatient with positive PCR test, Outpatient with negative PCR test, and Convalescent (individuals with a previous COVID infection) with positive PCR test and symptom free at least two weeks prior to sample collection.
The researchers first looked at the presence of antibodies toward the receptor binding domain (RBD) of the spike protein of SARS-CoV-2. Antibodies were present in 93% of the Inpatient+ group, 40% of the Outpatient+ group, 97% of the Convalescent+ group, and as expected, none were detected in the Outpatient- group. Next, they tested for the presence of ACE2 autoantibodies to determine if the presence of spike antibodies coincided. They found that ACE2 autoantibodies were present within the groups in a similar trend, suggesting that there could be a correlation between the development of SARS-CoV-2 spike RBD antibodies and ACE2 autoantibodies.
Antibodies: double-edged swords
Researchers also compared the amount and the activity of soluble ACE2 in patient plasma samples. They did not see significant differences in either case, which suggested there was not a defect in the expression of ACE2 following infection. Next, they performed an assay where samples of plasma with ACE2 autoantibodies were added to plasma samples that did not have ACE2 autoantibodies to determine if ACE2 activity was affected. The addition of ACE2 autoantibodies resulted in an overall decrease in ACE2 activity suggesting that patients with these autoantibodies suffer from a decrease in ACE2 activity. The loss of ACE2 activity could lead to an overactive inflammatory state which in turn could contribute to symptoms of long COVID.
While the authors could not definitively show a causal relationship between long COVID symptoms and ACE2 autoantibodies, they speculated that since ACE2 autoantibodies were detected in patients that had COVID-19 and since they were capable of inhibiting ACE2 activity, these autoantibodies might indeed be an underlying mechanism of long COVID. More research is needed to further flesh out this tale of ACE2 autoantibodies, but Arthur et al. have created a solid foundation. If further research does show a definitive link between long COVID and these autoantibodies, readily-available treatment options could help individuals suffering from long COVID. For now, we will have to wait and see what future data reveal about this story of the anti-hero ACE2 autoantibody.
Journal Article: Arthur, J., et al. Development of ACE2 autoantibodies after SARS-CoV-2 infection. PLOS ONE (2021). https://doi.org/10.1371/journal.pone.0257016
Cover image courtesy of @KO__images
